
Translate this page into:
Progression of corneal sub-epithelial infiltrates in a case of undertreated epidemic keratoconjunctivitis

-
Received: ,
Accepted: ,
How to cite this article: Ramatchandirane B, Syamala DD, Ganne P. Progression of corneal sub-epithelial infiltrates in a case of undertreated epidemic keratoconjunctivitis. Lat Am J Ophthalmol 2023:6:17.
Abstract
A 27-year-old lady presented with watering, redness, blurring of vision and foreign body sensation in right eye since 3 days. On slit lamp examination, there was conjunctival follicular reaction and two pin head sized subepithelial infiltrates (SEI) suggestive of epidemic keratoconjunctivitis. Patient was started with ganciclovir 0.15% ointment along with fluorometholone-tobramycin drops with which patient relieved off her symptoms in 1 week and then discontinued herself but recurred with the same symptoms in 1 month. Initial two SEIs were progressed to six which all were disappeared after restarting fluorometholone-tobramycin drops. Presences of SEIs require prompt management with topical steroid and adequate treatment is needed till it resolved completely thereby permanent scarring of the cornea can be avoided.
Keywords
Progression of subepithelial infiltrates
Subepithelial infiltrates
Epidemic keratoconjunctivitis
Topical steroids

INTRODUCTION
A 27-year-old lady presented with watering, redness, blurring of vision, and foreign body sensation in the right eye (RE) for 3 days following an episode of flu-like illness. Best corrected visual acuity (BCVA) was 20/40 (RE). Slit lamp examination showed conjunctival follicular reaction and two pinhead sized grayish lesions with a fluffy border in the central part of the right cornea (not staining with fluorescein dye) suggestive of sub epithelial infiltrates (SEI) [Figure 1a]. A clinical diagnosis of epidemic keratoconjunctivitis (EKC) was made and the patient was put on ganciclovir eye ointment (0.15%) 5 times a day along with a tapering dose of fluorometholone (0.1%) - tobramycin (0.3%) combination eye drops starting at 4 times a day and advised to follow-up 1 week later. The patient stopped treatment 1 week later since she was relieved off her symptoms. However, she came back with decreasing vision in the RE 1 month later. BCVA in the RE was 20/40. Slit lamp examination of her RE showed that the SEIs progressed and now there are six spots in the cornea [Figure 1b and c]. Treatment with fluorometholone (0.1%) - tobramycin (0.3%) combination eye drops was re-started at 4 times a day. At the end of 2 weeks, SEIs completed disappeared [Figure 1d] and BCVA improved to 20/20.
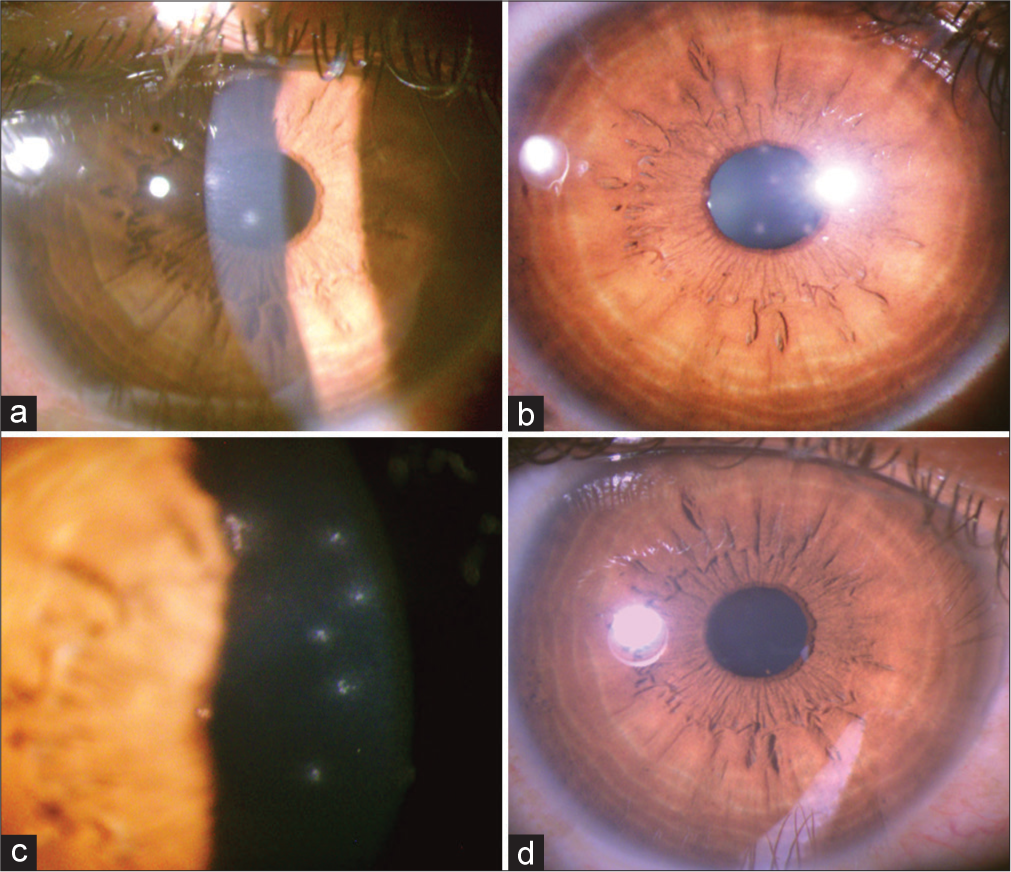
- The various stages of subepithelial infiltrates. (a) Slit lamp photograph shows two greyish white pinhead sized subepithelial infiltrates in the central cornea. (b and c) Slit lamp photograph shows progression of subepithelial infiltrates to six spots following discontinuation of steroid at 1 month follow-up. (d) Slit lamp photograph shows complete resolution of subepithelial infiltrates after re-starting steroid treatment.
DISCUSSION
SEI are pathognomonic for EKC.[1] These lesions develop because of the immune response of the host to the proliferating viral particles in the corneal sub-epithelial region.[2] The incidence of SEI following acute adenoviral EKC is reported to be between 49.1% and 80%.[3,4] Prompt resolution of these lesions with topical steroids is seen. However, recurrences have been noted after stopping steroids. Left untreated/ undertreated these lesions can progress to corneal scarring and cause significant visual morbidity.
CONCLUSION
This case report demonstrates the photographic documentation of the progression of SEIs in case of inadequate treatment and also emphasize about adequate treatment to avoid such untoward outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflict of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Epidemic keratoconjunctivitis: A review of current concepts in management. J Optom. 2013;6:69-74.
- [CrossRef] [Google Scholar]
- Cyclosporine a 0.05% eye drops for the treatment of subepithelial infiltrates after epidemic keratoconjunctivitis. BMC Ophthalmol. 2012;12:42.
- [CrossRef] [PubMed] [Google Scholar]
- Adenoviral keratoconjunctivitis in a tertiary care eye clinic. Cornea. 2006;25:199-202.
- [CrossRef] [PubMed] [Google Scholar]




